
Genetic analysis using the Oak Ridge National Lab supercomputer called the Summit has revealed an interesting new hypothesis that helps explain the disease progression of COVID-19. A September 1, 2020, Medium article1 by Thomas Smith reviewed the findings of what is now referred to as the bradykinin hypothesis.
As reported by Smith, the computer crunched data on more than 40,000 genes obtained from 17,000 genetic samples.
“Summit is the second-fastest computer in the world, but the process — which involved analyzing 2.5 billion genetic combinations — still took more than a week. When Summit was done, researchers analyzed the results. It was, in the words of Dr. Daniel Jacobson, lead researcher and chief scientist for computational systems biology at Oak Ridge, a ‘eureka moment.’”
The Bradykinin Hypothesis
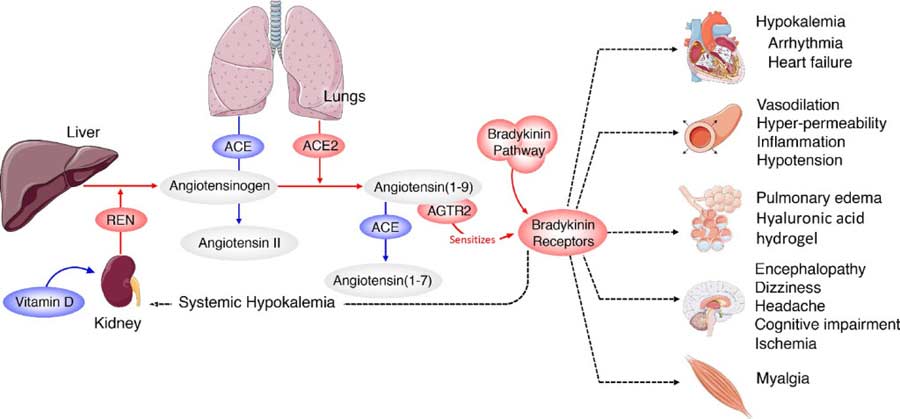
Bradykinin is a chemical that helps regulate your blood pressure and is controlled by your renin-angiotensin system (RAS). As explained in the Academic Press’ book on vitamin D (which has a significant impact on the RAS):2
“The renin-angiotensin system (RAS) is a central regulator of renal and cardiovascular functions. Over-activation of the RAS leads to renal and cardiovascular disorders, such as hypertension and chronic kidney disease, the major risk factors for stroke, myocardial infarction, congestive heart failure, progressive atherosclerosis, and renal failure.”
The bradykinin hypothesis provides a model that helps explain some of the more unusual symptoms of COVID-19, including its bizarre effects on the cardiovascular system. It also strengthens the hypothesis that vitamin D plays a really important role in the disease.
The findings3 were published in the journal eLife July 7, 2020. Based on this new hypothesis, the researchers also suggest more than 10 potential treatments, most of which are readily available drugs already approved by the U.S. Food and Drug Administration. I’ll review those later on.
As detailed in previous articles, your ACE2 receptors are the primary gateways of the virus, as the virus’ spike protein binds to the ACE2 receptor. As explained by Smith:4
“… COVID-19 infection generally begins when the virus enters the body through ACE2 receptors in the nose … The virus then proceeds through the body, entering cells in other places where ACE2 is also present: the intestines, kidneys, and heart. This likely accounts for at least some of the disease’s cardiac and GI symptoms.
But once Covid-19 has established itself in the body, things start to get really interesting … The data Summit analyzed shows that COVID-19 isn’t content to simply infect cells that already express lots of ACE2 receptors. Instead, it actively hijacks the body’s own systems, tricking it into upregulating ACE2 receptors in places where they’re usually expressed at low or medium levels, including the lungs.
In this sense, COVID-19 is like a burglar who slips in your unlocked second-floor window and starts to ransack your house. Once inside, though, they don’t just take your stuff — they also throw open all your doors and windows so their accomplices can rush in and help pillage more efficiently.”
Bradykinin Storm Likely Responsible for Lethal Effects
In addition to upregulating ACE2 receptors throughout your body, the SARS-CoV-2 virus also downregulates your body’s ability to degrade or break down bradykinin.
The end result is a bradykinin storm, and according to the researchers, this appears to be an important factor in many of COVID-19’s lethal effects, even more so than the cytokine storms associated with the disease. As bradykinin accumulates, the more serious COVID-19 symptoms appear.
Mounting clinical data suggest COVID-19 is actually primarily a vascular disease rather than a respiratory one, and runaway bradykinin buildup can help explain this.
How SARS-CoV-2 Attacks the Lungs
That said, COVID-19 certainly has a respiratory component, and it appears the virus attacks the lungs in more ways than one. For starters, bradykinin increases vascular permeability, essentially causing your blood vessels to leak fluid. In the lungs, this leads to fluid buildup that can trigger inflammation when immune cells also leak out into the lungs.
But the Summit data also show the virus uses yet another pathway, which raises production of hyaluronic acid (HLA) in your lungs. HLA has the ability to absorb more than 1,000 times its own weight in fluid, and when it combines with the built-up fluid in the lungs, the effect is devastating, as it ends up forming a thick hydrogel that makes breathing near-impossible.
When this happens — in severe cases — even mechanical ventilation becomes ineffective, as the alveoli in the lungs are simply too clogged with this gel-like substance that prevents oxygen uptake.
Note that the HLA produced in your lungs does not mean that using supplemental HLA is a bad strategy. It is only when HLA is produced locally in high concentrations in pathologic conditions like COVID-19 that it becomes problematic. Otherwise it has important physiologic benefits.
How SARS-CoV-2 Attacks Your Heart and Brain
SARS-CoV-2 can also affect heart function, causing arrhythmias and low blood pressure. About 1 in 5 COVID-19 patients requiring hospitalizations have experienced damage to their heart. Your heart has ACE2 receptors, so SARS-CoV-2 has the ability to infect your heart directly. Arrhythmias and low blood pressure can also be the result of a bradykinin storm.
In some cases, COVID-19 has also been known to trigger neurological symptoms such as dizziness, seizures, delirium and stroke, and this too can be explained by bradykinin buildup.
At high levels, bradykinin can lead to a breakdown of your blood-brain barrier, thereby allowing harmful compounds to flood your brain. Bradykinin itself also causes blood vessel leakage. Together, these effects can trigger inflammation, brain damage and a variety of neurological symptoms.
SARS-CoV-2 Mimics ACE Inhibiting Drugs
Interestingly, as reported by Smith:5
“Increased bradykinin levels could also account for other common COVID-19 symptoms. ACE inhibitors — a class of drugs used to treat high blood pressure — have a similar effect on the RAS system as COVID-19, increasing bradykinin levels.
In fact, Jacobson and his team note in their paper that ‘the virus … acts pharmacologically as an ACE inhibitor’ — almost directly mirroring the actions of these drugs.
By acting like a natural ACE inhibitor, COVID-19 may be causing the same effects that hypertensive patients sometimes get when they take blood pressure-lowering drugs. ACE inhibitors are known to cause a dry cough and fatigue, two textbook symptoms of COVID-19.
And they can potentially increase blood potassium levels, which has also been observed in COVID-19 patients. The similarities between ACE inhibitor side effects and COVID-19 symptoms strengthen the bradykinin hypothesis, the researchers say.”
Another side effect associated with ACE inhibiting drugs is the loss of smell and taste. This is also an early sign associated with SARS-CoV-2 infection, and it’s a primary symptom of zinc deficiency too.
Zinc, as explained in “Swiss Protocol for COVID — Quercetin and Zinc,” plays a vital role in immunity as well as in blood clotting, cell division, thyroid health, smell and taste, vision and wound healing, and can effectively inhibit viral replication.
Your body does not store zinc, and it’s poorly absorbed, which appears to be why the combination of zinc and zinc ionophores such as quercetin and hydroxychloroquine are so effective when taken at first symptoms.
Bradykinin Hypothesis Explains Other COVID-19 Symptoms Too
The bradykinin storm also helps explain other odd COVID-19 symptoms such as “COVID toes,” a condition in which your toes become swollen and bruised. This may be due to leaky vasculature in your toes.
As explained by Smith, it can also shed helpful light on the gender differences seen in COVID-19. Women tend to have a lower mortality rate than men, and this may be due to the fact that women have twice the level of certain proteins involved in the RAS system.
Potential Treatments
The good news is that if bradykinin storms are to blame, there are a number of already existing drugs that can help prevent bradykinin storms, either reducing bradykinin or blocking its receptors. As noted in the study:6
“Several interventional points (most of them already FDA-approved pharmaceuticals) could be explored with the goal of increasing ACE, decreasing BK [bradykinin], or blocking BK2 receptors.
Icatibant is a BKB2R antagonist whereas Ecallantide acts to inhibit KLKB1, reducing levels of BK production. Androgens (danazol and stanasolol) increase SERPING1, although the side effects likely make these undesirable, but recombinant forms of SERPING1 could be administered to reduce BK levels.
It should be noted that any intervention may need to be timed correctly given that REN levels rise on a diurnal cycle, peaking at 4AM which corresponds with the commonly reported worsening of COVID-19 symptoms at night …
4-methylumbelliferone (Hymecromone) is a potent inhibitor of HAS1, HAS2, and HAS3 gene expression and results in the suppression of the production of hyaluronan in an ARDS model.
Hymecromone (4-methylumbelliferone) is approved for use in Asia and Europe for the treatment of biliary spasm. However, it can cause diarrhea with subsequent hypokalemia, so considerable caution should be used if this were to be tried with COVID-19 patients … Timbetasin may reduce COVID-19 related coagulopathies by increasing fibrinolysis.”
However, please understand that taking these drugs is absolutely not my recommendation. These are simply the conventional strategies that can be used if this hypothesis is correct.
Why on earth would we use dangerous drugs like these for a disease that they have not been tested on when we have so many other safe, inexpensive and highly effective interventions for COVID-19? Strategies like nebulized peroxide, ozone, molecular hydrogen, exogenous ketones, and quercetin with zinc.
Evidence for Vitamin D Strengthens
The researchers also highlight the usefulness of vitamin D, noting that “Another approach would be the modulation of REN levels via Vitamin D supplementation …” Vitamin D is involved in the RAS system,7,8,9 and can reduce a compound called renin (REN), thereby preventing a deadly bradykinin storm. Renin is an endopeptidase, the function of which is to generate angiotensin 1 from angiotensinogen in your plasma.
Several investigations have highlighted the apparent influence of vitamin D in COVID-19 incidence, severity and mortality, and its effects on RAS further strengthens the idea that vitamin D may be a crucial component in your COVID-19 defense arsenal.
As explained in the 2004 paper,10 “Vitamin D: A Negative Endocrine Regulator of the Renin-Angiotensin System and Blood Pressure,” when the RAS system is inappropriately activated, high blood pressure can result.
One factor that influences your RAS is your vitamin D level, as it suppresses renin biosynthesis. If you are vitamin D deficient, your renin expression is stimulated, and based on the latest data, that may render you more prone to bradykinin storm.
The Evidence for Vitamin D
In a November 1, 2020 commentary11 in the journal Metabolism Clinical and Experimental, JoAnn Manson and Shari Bassuk call for the elimination of vitamin D deficiency to effectively squelch the COVID-19 pandemic, noting that 23.3% of the total U.S. population have insufficient or deficient vitamin D levels, with people of color having disproportionately lower levels than non-Hispanic whites.
They list several types of studies showing vitamin D deficiency is “an important modifiable risk factor for COVID-19,” including:12
• Laboratory studies that demonstrate how vitamin D helps regulate immune function and the RAS, and modulate inflammatory responses to infection.
• Ecologic studies showing populations with lower vitamin D levels or lower UVB radiation exposure have higher COVID-19 mortality,13,14,15 and the fact that people identified as being at greatest risk for COVID-19 hospitalization and death (people of color, the elderly, nursing home residents and those with comorbidities such as obesity, vascular conditions and chronic kidney disease) also have a higher risk of vitamin D deficiency.
A pilot randomized clinical study16,17 published online August 29, 2020, found hospitalized COVID-19 patients in Spain who were given supplemental vitamin D (calcifediol) in addition to standard of care — which included the use of hydroxychloroquine and azithromycin — had significantly lower intensive care unit admissions.
Patients in the vitamin D arm received 532 micrograms of calcifediol on the day of admission (equivalent to 106,400 IUs of vitamin D18) followed by 266 mcg on Days 3 and 7 (equivalent to 53,200 IUs19). After that, they received 266 mcg once a week until discharge, ICU admission or death.
Of those receiving calcifediol, only 2% required ICU admission, compared to 50% of those who did not get calcifediol. None of those given vitamin D supplementation died, and all were discharged without complications.
• Observational studies showing low vitamin D levels are associated with a greater risk of testing positive for SARS-CoV-2 and contracting acute respiratory infections.
Most recently, a September 3, 2020 JAMA study20 reported that people who tested positive for SARS-CoV-2 were 1.77 times more likely to be deficient in vitamin D than those who tested negative for the virus.
• Randomized clinical trials showing vitamin D inhibits respiratory tract infections, especially in those with lower vitamin D levels at baseline.
REALLY IMPORTANT: Optimize Your Vitamin D Level Now
For years, I’ve stressed the importance of optimizing your vitamin D level, especially in anticipation of flu season, and it seems clear it can go a long way toward protecting yourself against COVID-19 as well.
Aside from what’s already been mentioned, vitamin D also helps Type II cells in your lungs produce surfactant that aids in fluid clearance. When you’re vitamin D deficient, your entire RAS is deranged or dysfunctional, thereby raising your risk of both bradykinin storm and cytokine storm.
In closing, experts have been warning that SARS-CoV-2 may reemerge in the fall when temperatures and humidity levels drop, thereby increasing the virus’ transmissibility.
Now is the time to check your vitamin D level and start taking action to raise it if you’re below 60 ng/mL. An easy and cost-effective way of measuring your vitamin D level is to order GrassrootsHealth’s vitamin D testing kit and learn more about vitamin D and its impact on your health.
Knowledge is empowerment, and that is particularly true during this pandemic. To learn more about the influence of vitamin D on your health in general and COVID-19 in particular, see my vitamin D report.